A sensitive, accurate and standardized method for MRD detection and monitoring
The clonoSEQ® Assay is a robust, highly-validated tool for identifying and monitoring measurable residual disease (MRD) in lymphoid malignancies.[1] Across a variety of large, multi-center clinical trials, clonoSEQ has generated a wealth of peer-reviewed clinical evidence in disease states including multiple myeloma (MM), B-cell acute lymphoblastic leukemia (ALL), and chronic lymphocyticleukemia (CLL).[2,3]
Review specific data for:
Multiple Myeloma
Data Spotlight
COLLABORATORS
Maria-Victoria Mateos, University of Salamanca, Salamanca, Spain
PATIENTS
569 relapsed and refractory patients assessed for MRD by clonoSEQ at the time of suspected complete response (CR)
STUDY OBJECTIVE
Evaluate use of clonoSEQ MRD testing for prognostic evaluation by correlating MRD results to PFS.[4]

PROGNOSTIC VALUE
The clonoSEQ Assay can predict progression-free survival in myeloma patients
MRD negativity* (as measured by clonoSEQ at 10-5 threshold) was associated with longer PFS than MRD positivity, regardless of the treatment received
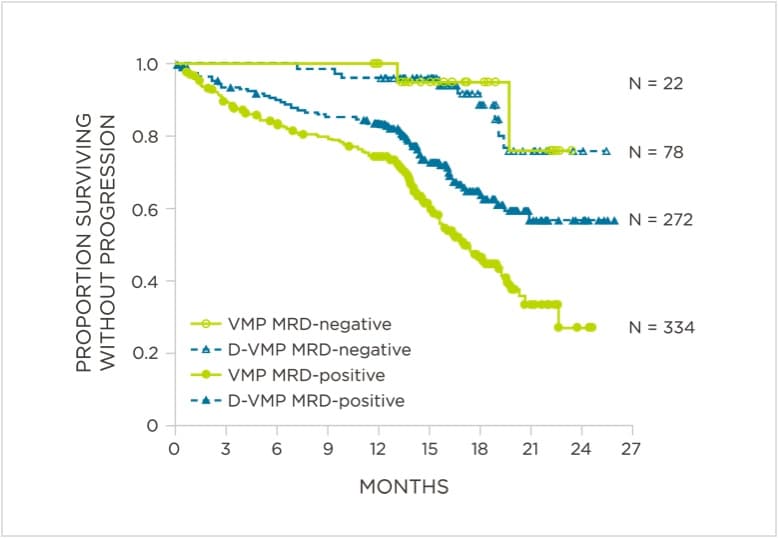
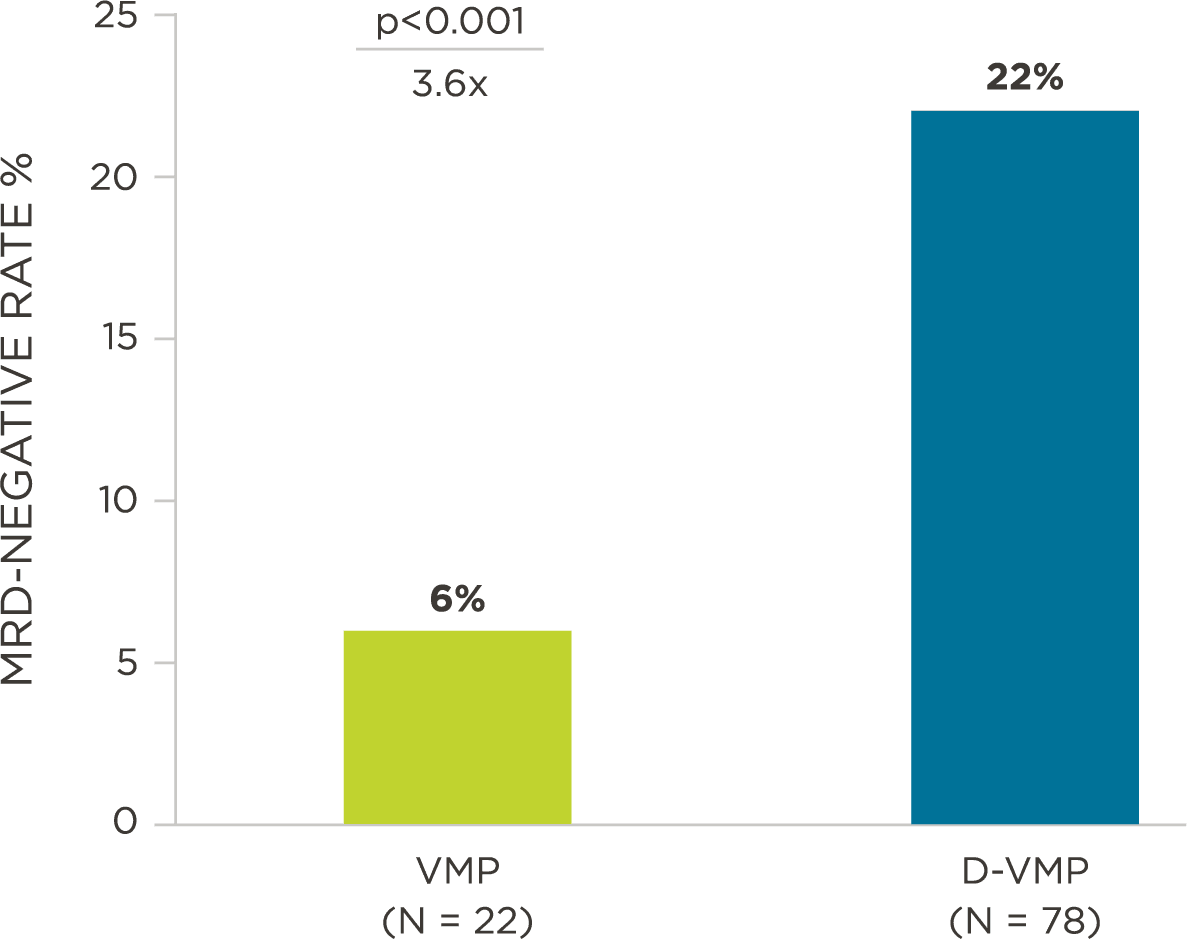
In the ALCYONE (NCT02195479) study of 706 patients with newly diagnosed, transplant-ineligible multiple myeloma, patients received bortezomib, melphalan, and prednisone (VMP) with or without daratumumab (D-VMP). Patients were assessed by clonoSEQ (at a sensitivity level of 10-5) at study screening, and time of CR/sCR, as well as at 12, 18, 24, and 30 months in patients who had achieved a CR/sCR following initiation of induction. After 18 months of follow-up, the proportion of MRD-negative patients in the experimental treatment arm was more than three times higher than in the control group (22.3% versus 6.2%, P<0.001; Figure 1). Additionally, regardless of treatment arm, MRD-negative patients had longer PFS than MRD-positive patients (Figure 2).[5] The MRD negativity rate data from this study has been incorporated in an FDA-approved product label for the treatment of newly-diagnosed, transplant-ineligible multiple myeloma patients.[6]
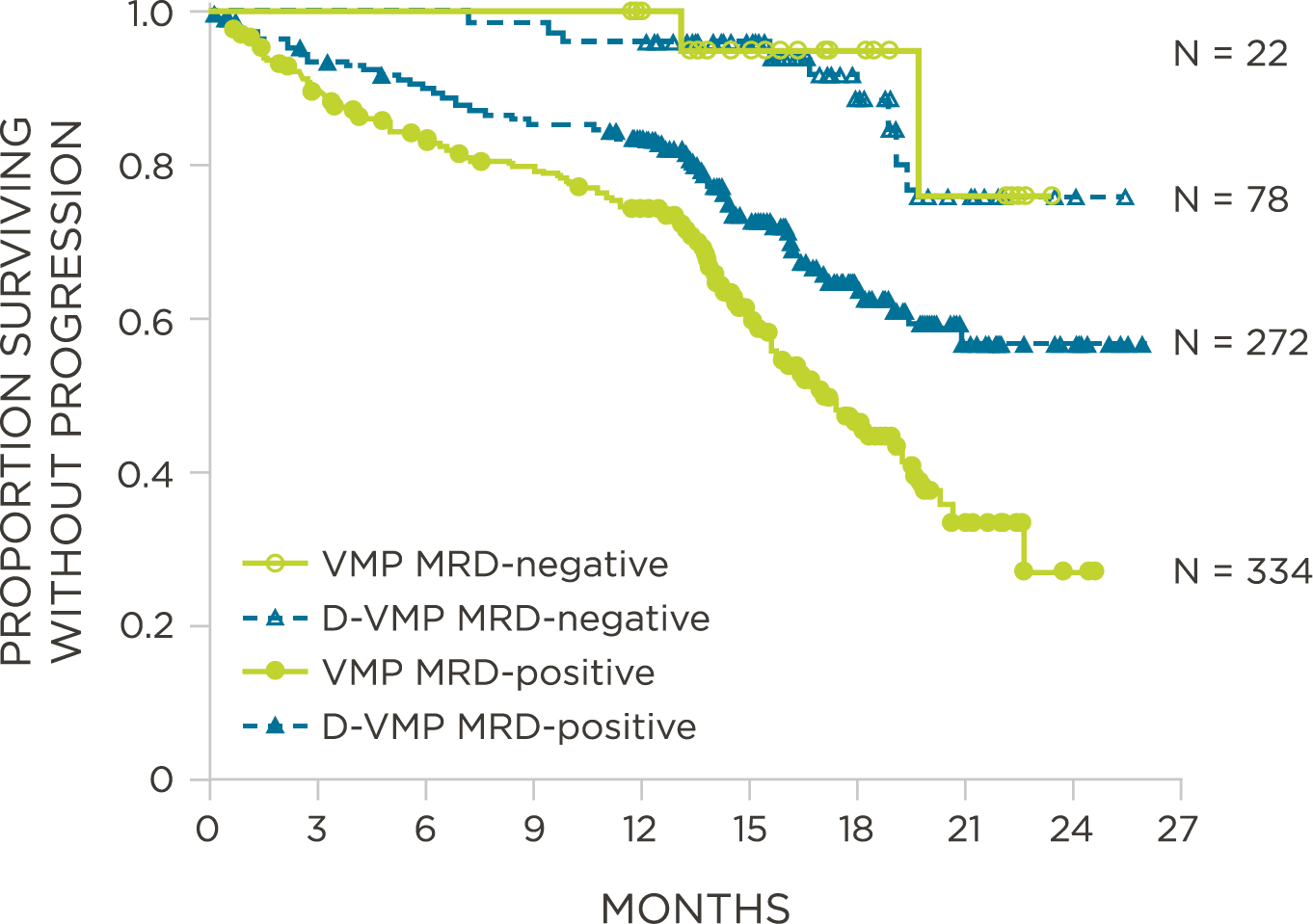
clonoSEQ MRD-negative patients have longer progression-free survival
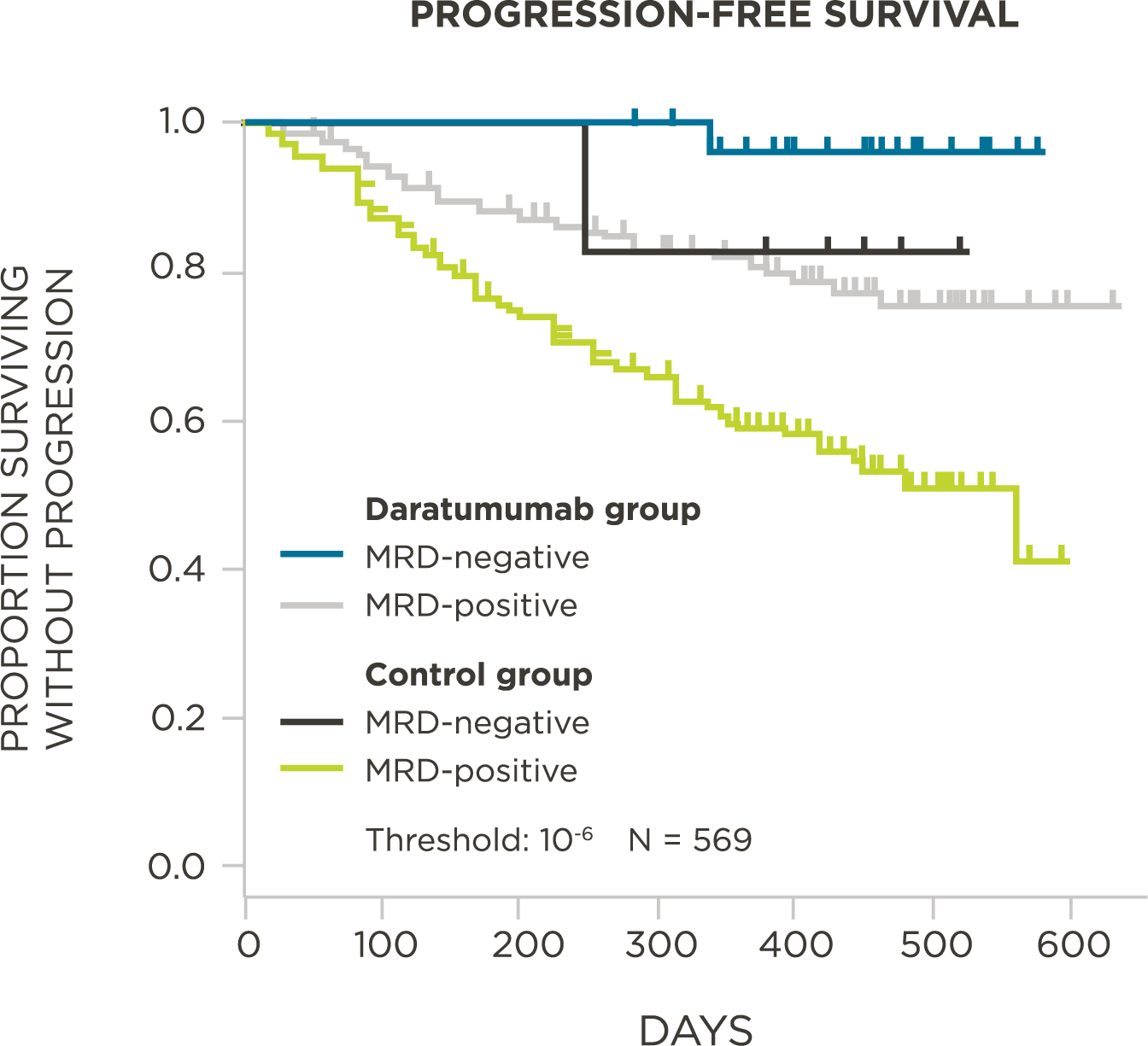
The POLLUX study assessed 569 relapsed and refractory multiple myeloma patients to determine if the addition of daratumumab to lenalidomide and dexamethasone (Rd) resulted in prolonged progression-free survival. MRD was assessed at three MRD thresholds (10-4 to 10-6) by clonoSEQ at the time of suspected complete response (CR). At three evaluated thresholds, MRD negativity by clonoSEQ was associated with longer PFS relative to MRD positivity (Figure 3, 10-6 threshold shown). Additionally, the rate of MRD negativity at all evaluated thresholds (10-4, 10-5, 10-6) was significantly higher in the experimental treatment arm than in the control arm (by 3-5x). Specifically, at an MRD threshold of 10-5, the rate of MRD negativity was 22.4% in the experimental group (DRd) versus 4.6% in the control group (Rd; P<0.001).[7]
Peer-reviewed publications show advantages to using clonoSEQ in Multiple Myeloma:
MRD assessment by clonoSEQ predicts time to tumor progression (TTP) and overall survival (OS).[8]
View More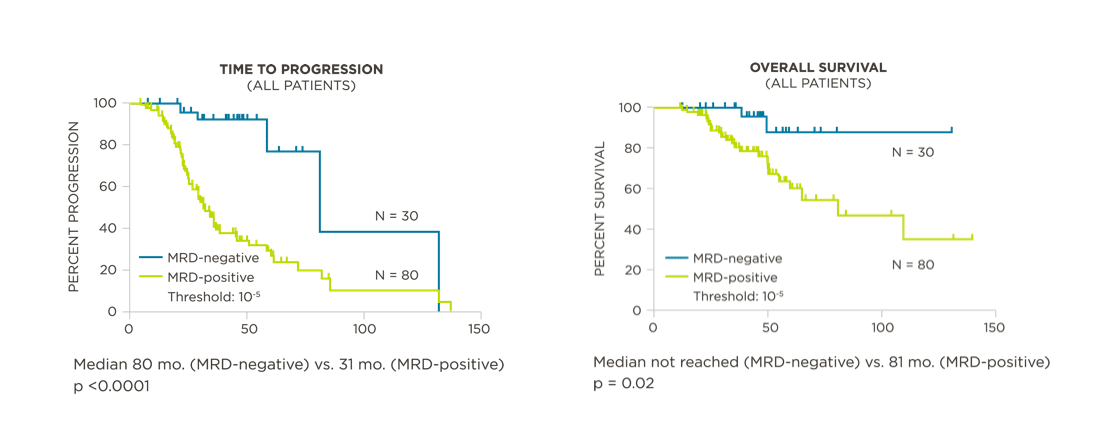
PROGNOSTIC VALUE
The clonoSEQ Assay has prognostic value in Multiple Myeloma
MRD by NGS predicts time to tumor progression and overall survival
A study of 133 patients on GEM clinical trials (GEM00, GEM05, and GEM2010) found that MRD assessment by NGS was prognostic for time to progression (TTP; Figure 4) and overall survival (OS; Figure 5).[8]
- Patients in a CR and MRD negative had longer TTP than patients in a CR who were MRD positive.[8]
- clonoSEQ MRD identified trackable sequences in 121/133 patients (91%).[8]
- There were 82 concordant MRD results between NGS and flow cytometry. There were 17 discordant MRD cases: 12 were NGS MRD-positive and flow MRD-negative; 5 were NGS MRD-negative and flow MRD-positive.
MRD negativity when assessed pre- and post-maintenance at deeper sensitivity correlated with improved outcomes.
View More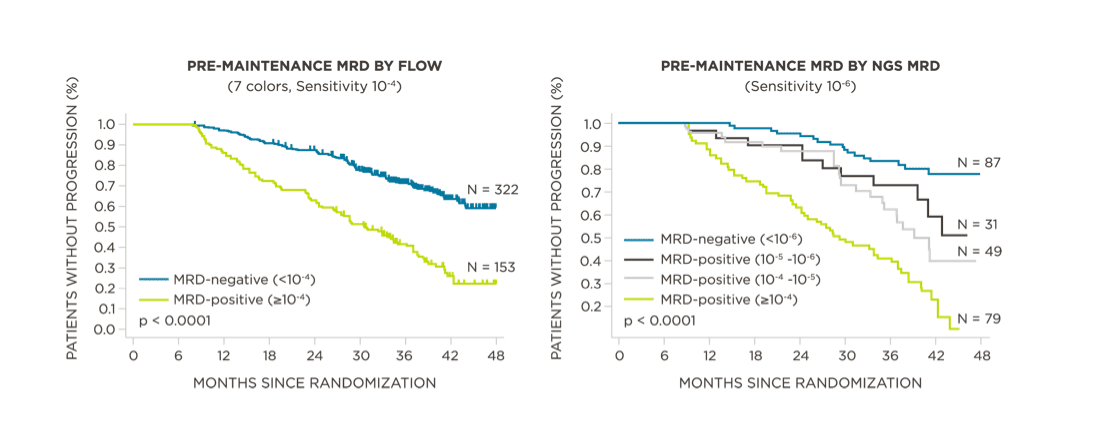
SENSITIVITY MATTERS
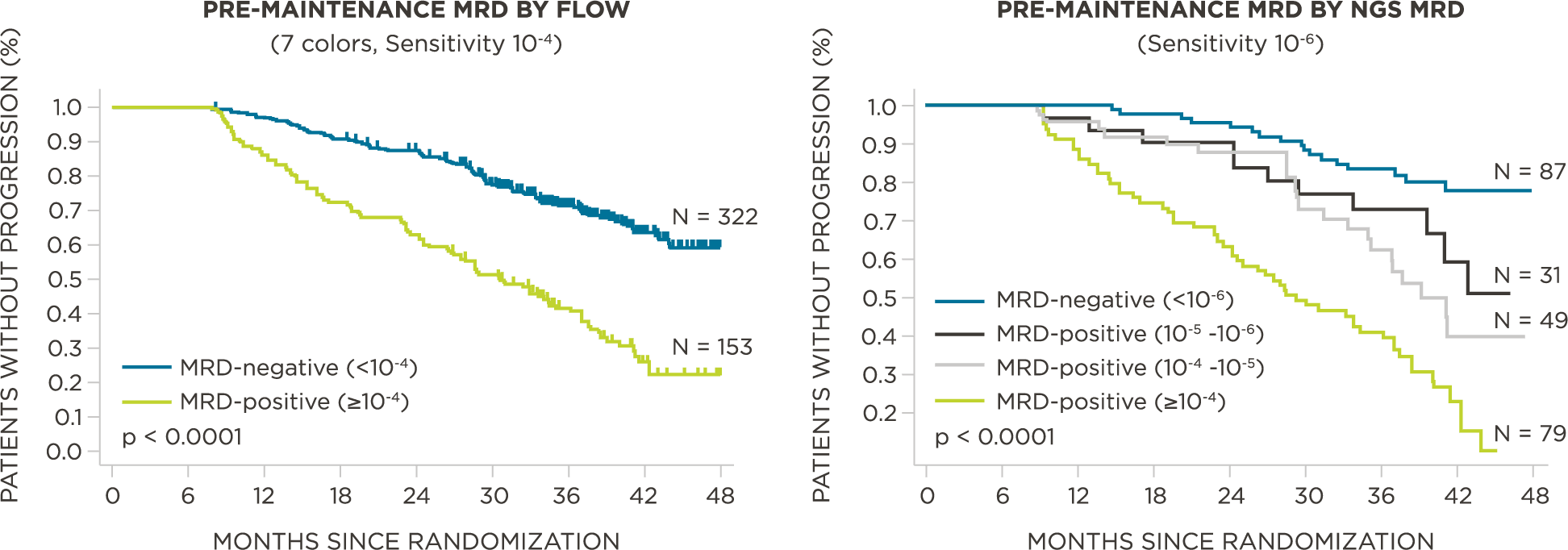
MRD negativity when assessed pre- and post-maintenance at deeper sensitivity correlated with improved outcomes
Better outcomes for patients who achieve lower levels of disease burden (deeper response) pre-maintenance
When assessing MRD by clonoSEQ, pre-maintenance, patients (N=246) were stratified by level of MRD detected (≥10-4, 10-4 – 10-5, 10-5 – 10-6, <10-6). Patients with the deepest level of MRD negativity (<10-6), had superior PFS compared to clonoSEQ MRD-positive patients with disease >10-6 (P<0.0001, Figure 6).[9]
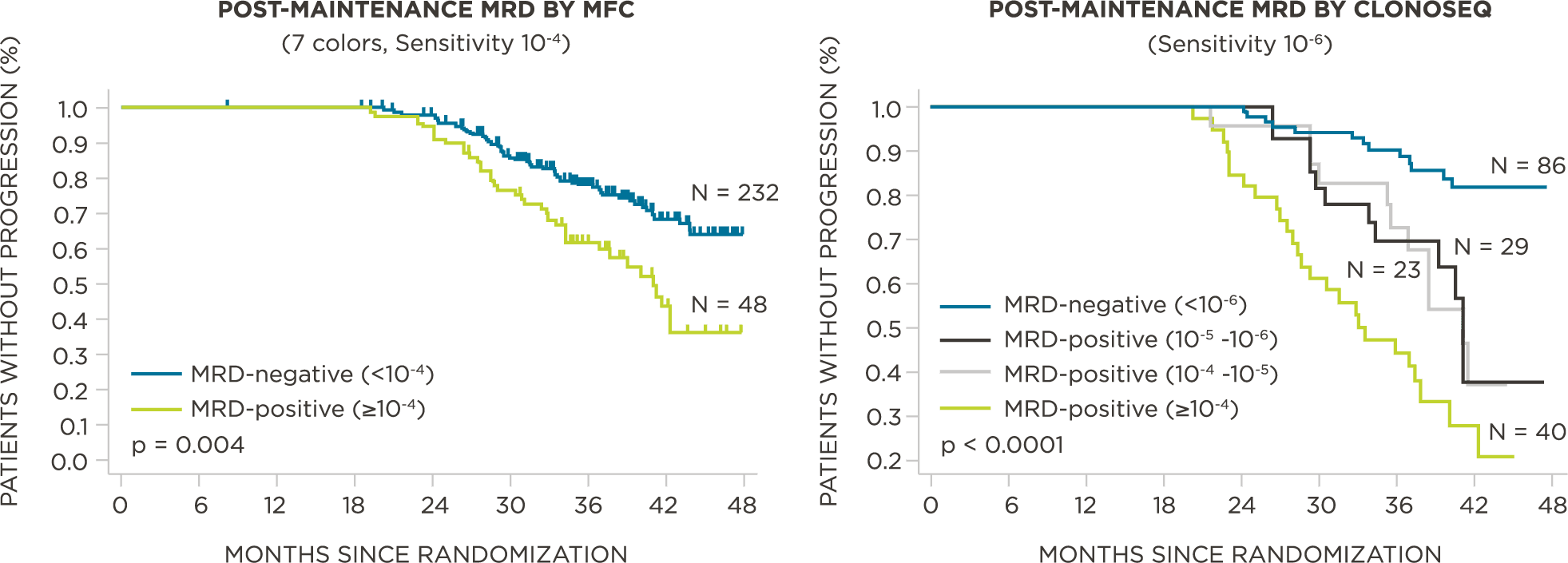
Better outcomes for patients who achieve lower levels of disease burden (deeper response) post-maintenance
When assessing MRD by clonoSEQ post-maintenance, patients (N=178) were stratified by level of MRD (≥10-4, 10-4 – 10-5, 10-5 – 10-6, <10-6). Patients with the deepest level of MRD negativity (<10-6) had superior PFS compared to clonoSEQ MRD-positive patients with disease >10-6 (P<0.0001, Figure 7).[9]
clonoSEQ MRD testing identified additional MRD-positive patients who were MRD-negative by flow cytometry in this study.
View More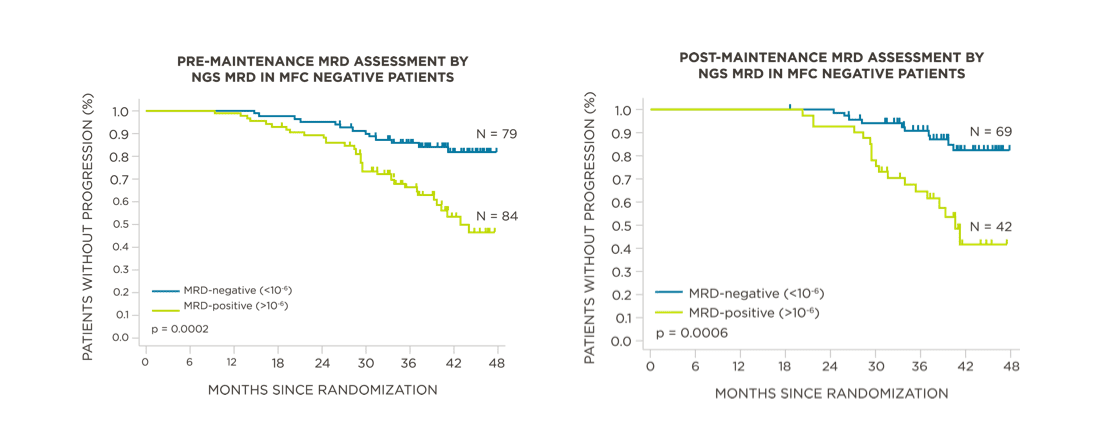
ADDITIONAL PATIENTS CAPTURED WITH CLONOSEQ MRD DETECTION
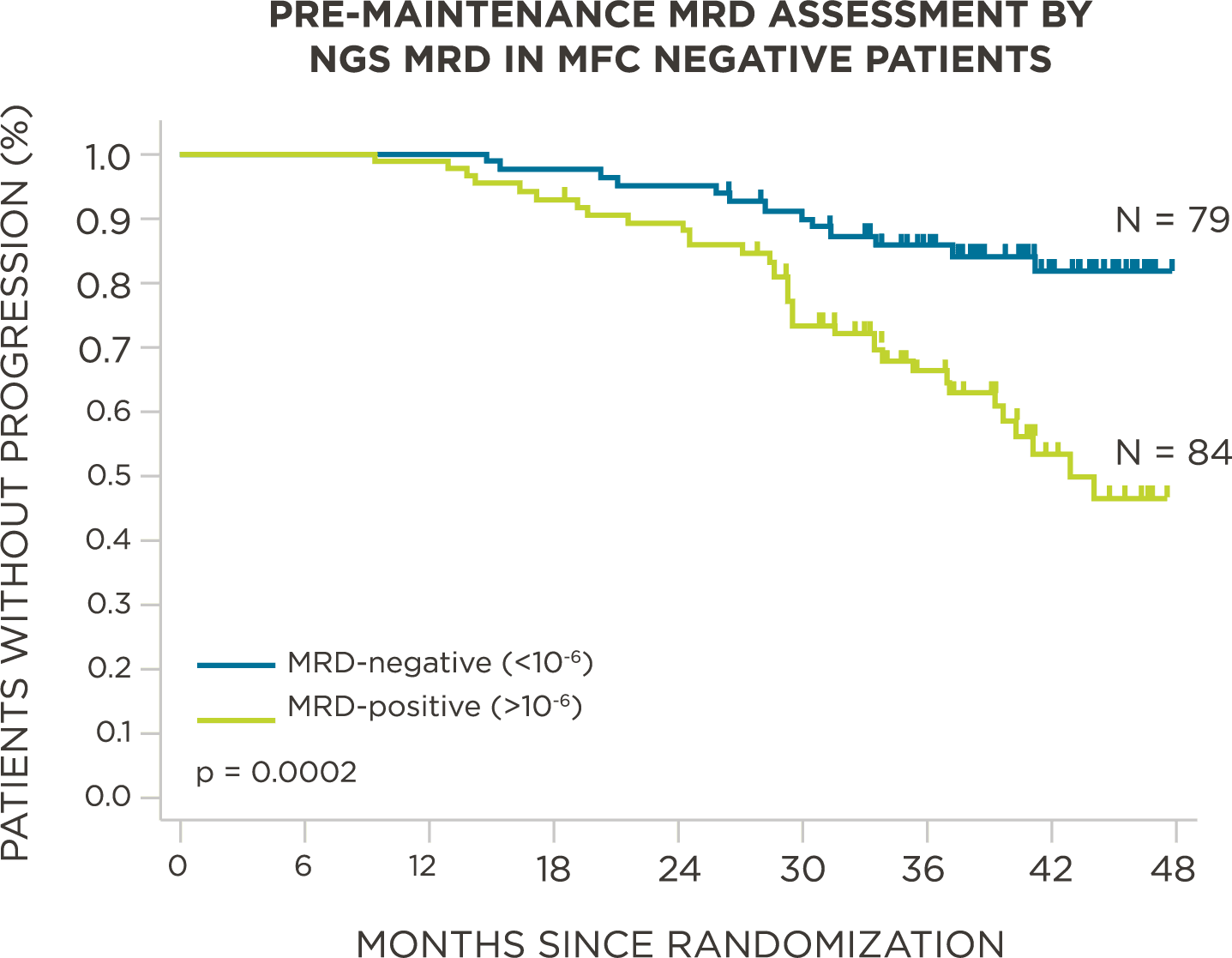
clonoSEQ MRD testing identified additional MRD-positive patients who were MRD-negative by flow cytometry in this study
Additional 84 MRD-positive patients captured pre-maintenance
In a study evaluating MRD in 475 patients, 322 patients had no detectable disease by flow cytometry, of which 163 patients were assessed by clonoSEQ. Of the clonoSEQ-assessed patients, 84 were identified as MRD-positive. These 84 patients had worse PFS compared to patients who had no detectable MRD by flow and were NGS MRD-negative (P=0.0002, Figure 8).[9]
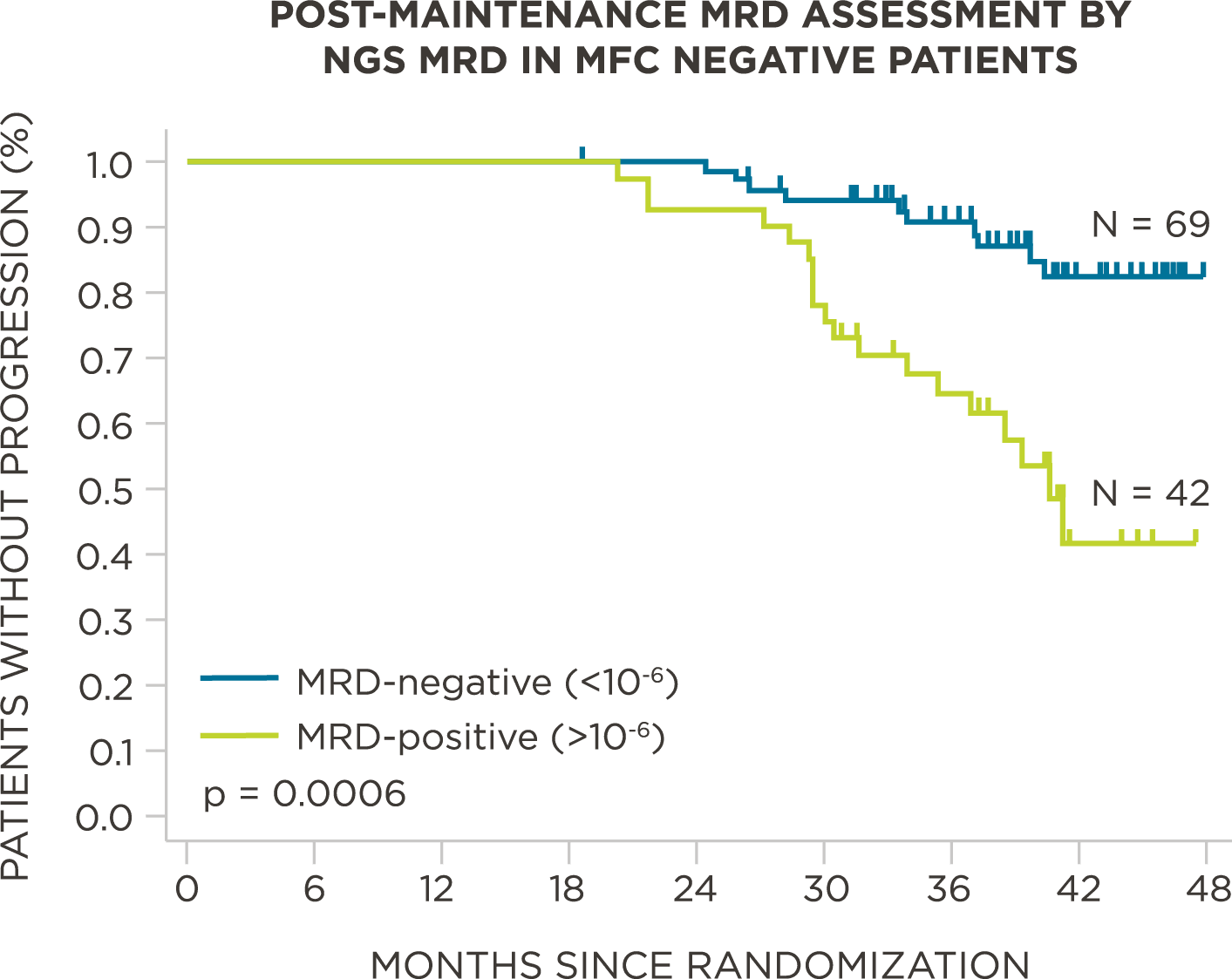
Additional 42 MRD-positive patients captured post-maintenance
Post-maintenance, 232 patients had no detectable MRD by flow cytometry, of which 111 were then assessed by clonoSEQ. Of these 111 patients, 42 were identified as MRD-positive by clonoSEQ. These patients had worse PFS compared to patients who were MRD-negative by flow and clonoSEQ (P=0.0006, Figure 9).[9]
Download Myeloma Clinical Data
Download our Multiple Myeloma clinical data summary to explore and share the data.
VIEW PDFReview NCCN Guidelines®
Access the NCCN Guidelines.
GUIDELINESAcute Lymphoblastic Leukemia
Data Spotlight
PATIENT POPULATION:
579 pediatric patients were assessed for MRD at baseline and end of induction (Day 29)
STUDY OBJECTIVE:
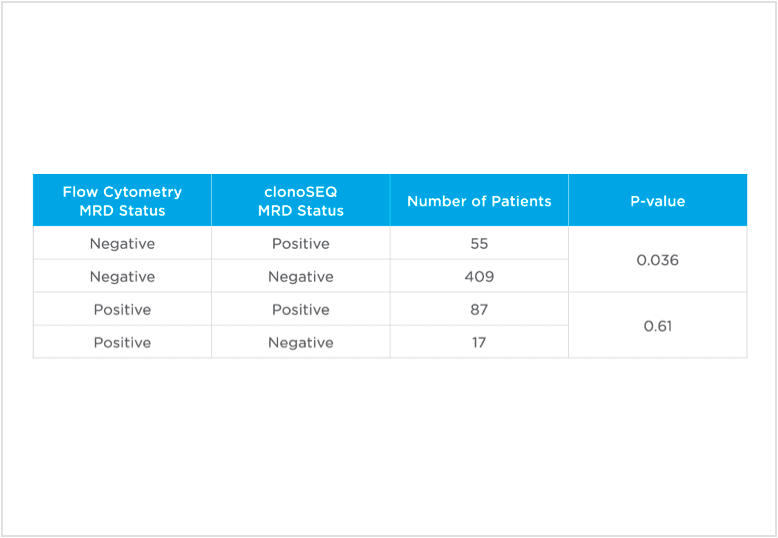
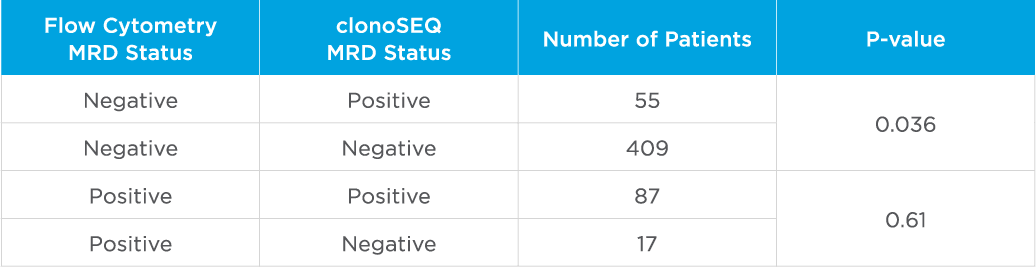
Evaluate non-inferiority of clonoSEQ to flow cytometry using an MRD threshold of 10-4 and understand if increased sensitivity of clonoSEQ identifies additional patients with residual disease compared to flow cytometry. Assessment of MRD at end of induction showed that sequencing-based MRD detection identified an additional 55 patients who were MRD-positive by the clonoSEQ Assay and MRD-negative by flow cytometry (p=0.036).[3]
ADDITIONAL PATIENTS CAPTURED WITH CLONOSEQ MRD DETECTION
The sensitivity and specificity of clonoSEQ MRD enables robust detection of disease
Additional 55 MRD-positive patients captured
A study evaluated MRD in the bone marrow of 579 pediatric ALL patients. Next-generation sequencing MRD detection identified an additional 55 patients who were MRD-positive by the clonoSEQ Assay and MRD negative* by flow cytometry at an MRD threshold of 10-4. 17 patients were identified as MRD-positive by flow cytometry and MRD-negative by clonoSEQ at a sensitivity of 10-4 (Table 1).[3] When assessing MRD at a threshold of 10-5, clonoSEQ identified an additional 87 patients with disease who were MRD-negative by flow cytometry.[3]
clonoSEQ MRD demonstrates ability to predict event-free survival (EFS) in pediatric ALL
This study demonstrated that 55 patients who had no detectable MRD by flow cytometry and who were MRD-positive by NGS had a worse EFS than those who were MRD-negative by NGS and had no detectable MRD by flow cytometry (threshold of 10-4). Using an MRD cutoff level of 10-4, flow cytometry identified 17 patients as MRD-positive that NGS identified as MRD-negative. When those 17 patients were assessed at an MRD cutoff level of 10-5, NGS identified residual disease in 11 of these patients. Additionally, NGS MRD (threshold of 10-4) was able to predict EFS in the standard risk subgroup. Patients who were NGS MRD-negative had longer EFS compared to the NGS MRD-positive patients (P=0.0226).[3]
Peer-reviewed publications show advantages to using clonoSEQ in ALL:
In one study, clonoSEQ was shown to be superior to flow cytometry in predicting post treatment relapse and survival.[13]
View More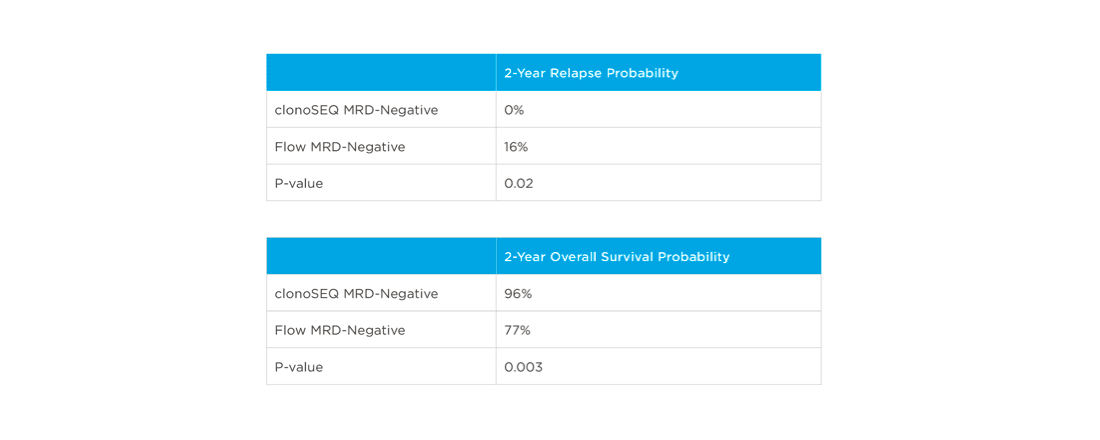
In one study, clonoSEQ was shown to be superior to flow cytometry in predicting post treatment relapse and survival.<sup>[13]</sup>
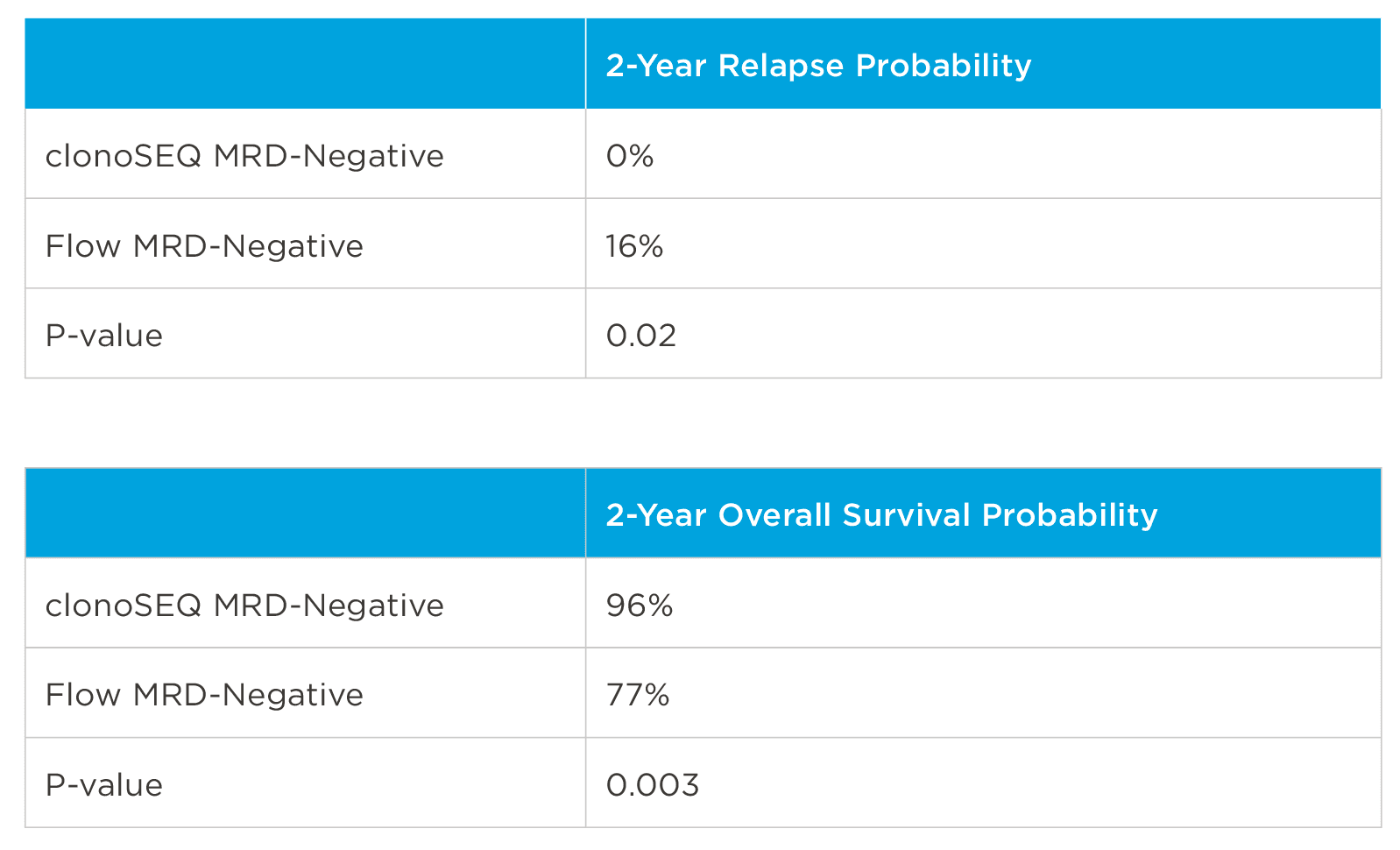
clonoSEQ MRD assessment pre-transplant may predict relapse and overall survival
In this analysis of pre-transplant bone marrow samples from 41 pediatric patients with ALL, it was found that clonoSEQ MRD detection predicted relapse and overall survival post-allogeneic transplant significantly better than 6-color flow cytometry (Table 2).[13]
clonoSEQ may be used to predict relapse and disease free survival in the post-transplant setting.[13]
View More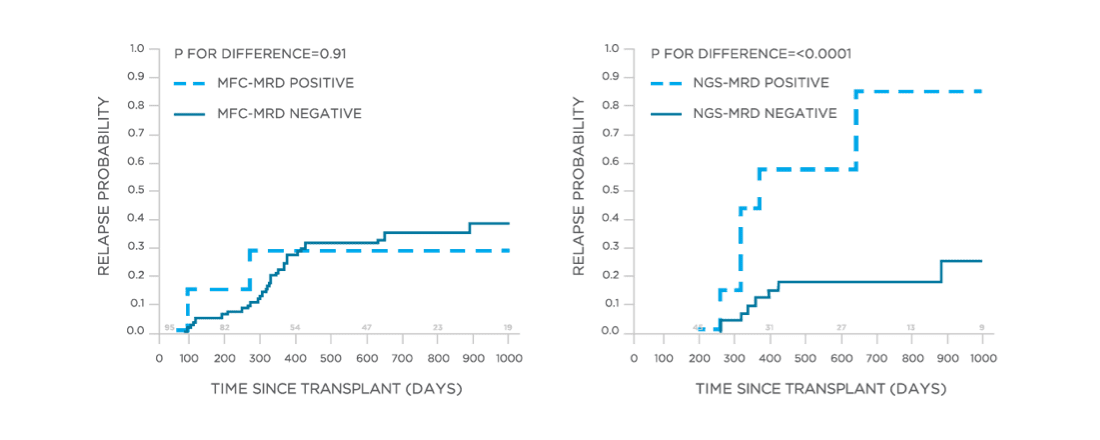
PROGNOSTIC VALUE
clonoSEQ MRD assessment has demonstrated prognostic value post-transplant in the pediatric and adult ALL settings
Analysis of bone marrow samples from 53 pediatric patients analyzed post-allogeneic transplant showed that clonoSEQ may be used to predict relapse. In the case of discordant MRD determinations, there were 11 patients identified as clonoSEQ MRD-positive and flow cytometry MRD-negative and 3 patients identified as clonoSEQ MRD-negative and flow cytometry MRD-positive.[13]
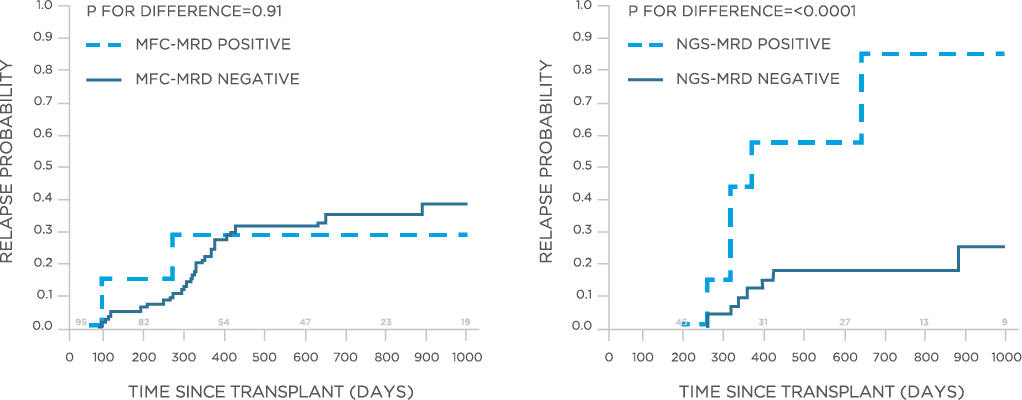
Strong predictive power
One month after transplant, flow cytometry was unable to distinguish between patients who ultimately relapsed and those who did not (p=0.91; Figure 3). NGS MRD showed an estimated relapse probability of 67% in MRD-positive patients vs. 25% in MRD-negative patients (p=0.01).[13]
Long range predictive power
Better predictive power of post-transplant NGS MRD detection vs. flow cytometry continued at day 100 and 8 months post-transplant.[13]
clonoSEQ is concordant with traditional methods for MRD detection and offers increased sensitivity.[12]
View More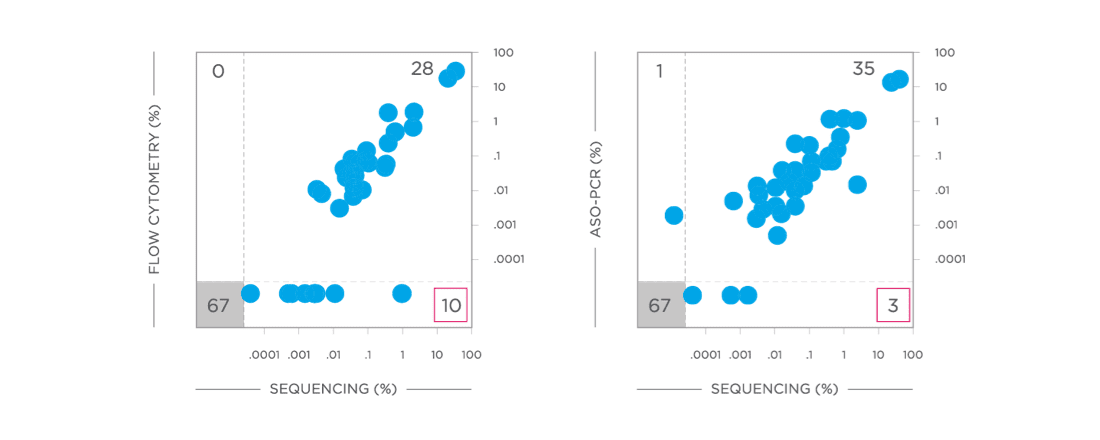
CONCORDANCE
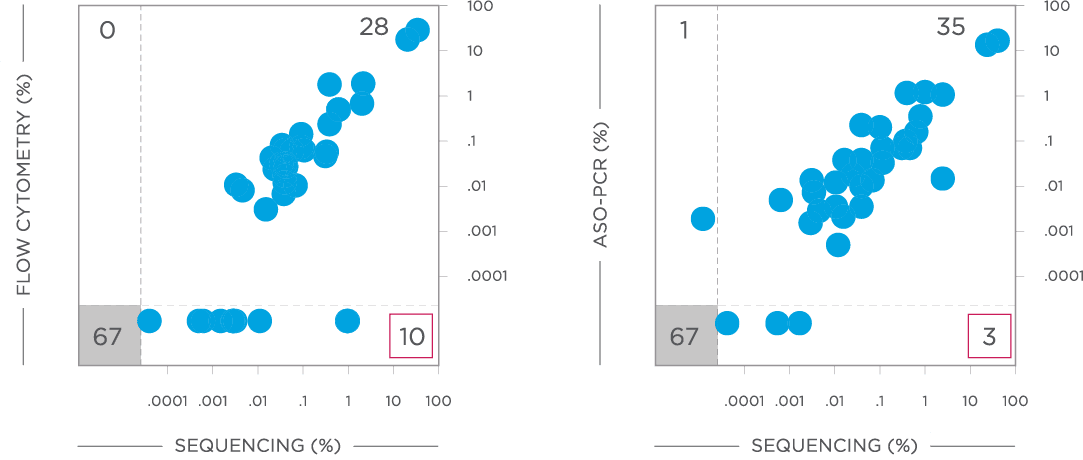
The clonoSEQ Assay is highly concordant with traditional MRD detection methods in ALL
In a study of more than 100 pediatric ALL patients, the clonoSEQ Assay showed quantitative concordance with both flow cytometry and allelespecific oligonucleotide PCR (ASO-PCR; Figure 2).[12]
Increased sensitivity
The clonoSEQ Assay was able to detect additional patients with disease present below the detection limits of flow cytometry (N=10) and ASO-PCR (N=3), respectively (Figure 2, red boxes).[12] ASO-PCR identified one patient with residual disease that was MRD-negative by clonoSEQ.[12]
Download ALL Clinical Data
Download our Acute Lymphoblastic Leukemia clinical data summary to explore and share the data.
VIEW PDFReview NCCN Guidelines®
Access the NCCN Guidelines.
GUIDELINES
ABILITY TO PREDICT CLINICAL OUTCOMES
clonoSEQ predicts outcomes three months after the completion of therapy
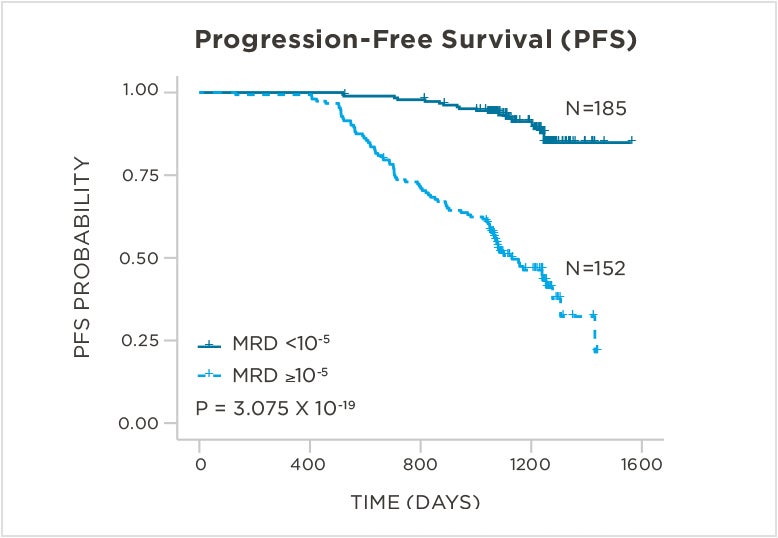
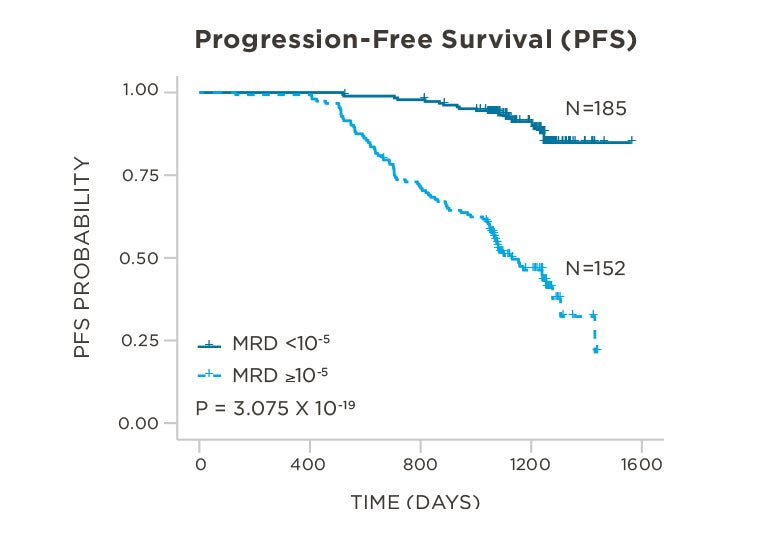
clonoSEQ can predict progression free survival
The CLL14 study assessed the combination of obinatuzumab plus venetoclax versus obinatuzumab plus chlorambucil in previously untreated CLL patients with coexisting conditions. MRD was assessed in peripheral blood samples from 337 patients three months after completion of therapy using an MRD threshold of 10-5. U-MRD by clonoSEQ significantly predicted progression-free survival (PFS; P = 3.075 x 10-19; Figure 1) with a 6.64-fold higher event risk in MRD-positive patients compared to U-MRD patients (95% CI: 3.65-12.1).[1]
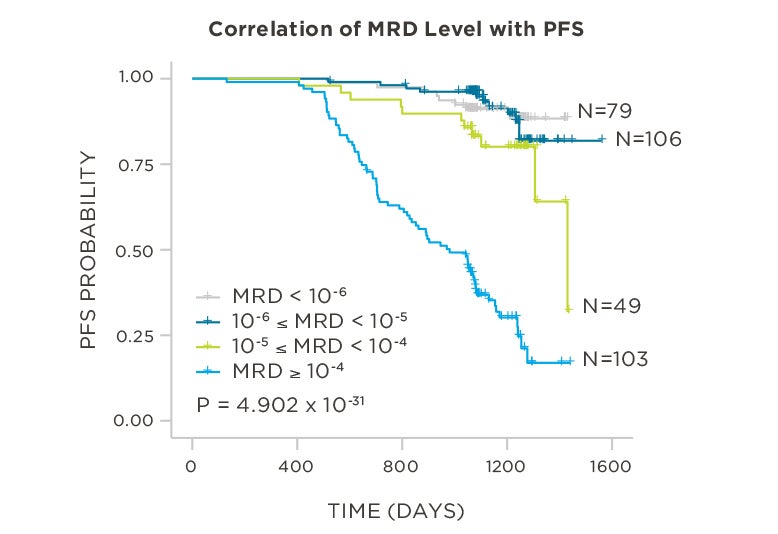
Lower levels of MRD are correlated with better outcomes
When assessing the correlation between clinical outcomes and continuous clonoSEQ MRD measurements (vs. a pre-definied sensitivity threshold), a patient’s risk of an event was shown to increase by 2.15-fold for every 10-fold increase in MRD (95% CI: 1.86-2.48).
Patients with U-MRD or very low levels of MRD detected by clonoSEQ have the best outcomes. Patients with clonoSEQ MRD < 10-6 or between 10-6 and 10-5 have the longest PFS, followed by patients with MRD between 10-5 and 10-4 and patients with MRD ≥ 10-4 (P = 4.902 x 10-31).
These data demonstrate that patients with MRD < 10-5 have better outcomes than patients with MRD ≥ 10-5, and that increasing MRD levels above 10-5 are associated with an increased risk of disease progression within the follow-up time of this study.[1]
Clinical studies show advantages to using clonoSEQ in CLL:
clonoSEQ predicts outcomes in both bone marrow and peripheral blood samples.
View More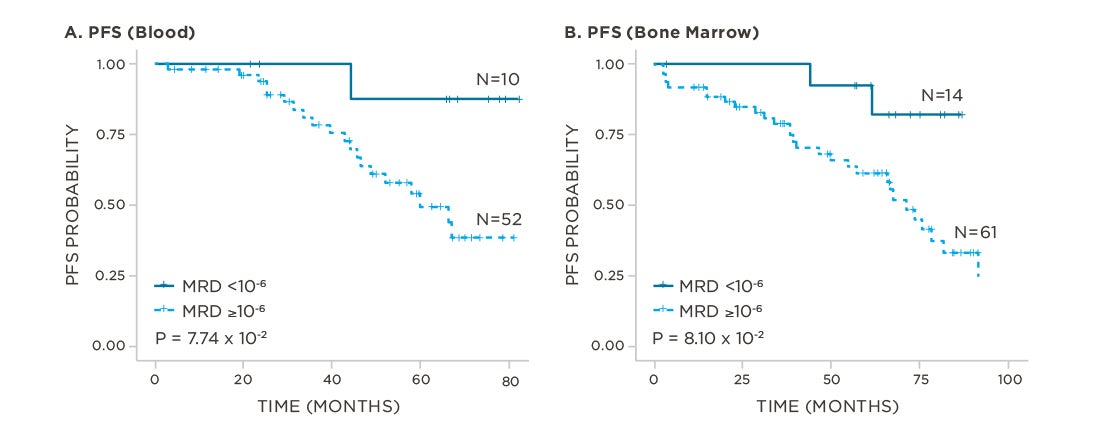
CONCORDANCE BETWEEN BLOOD AND BONE MARROW
clonoSEQ predicts outcomes in both bone marrow and peripheral blood samples
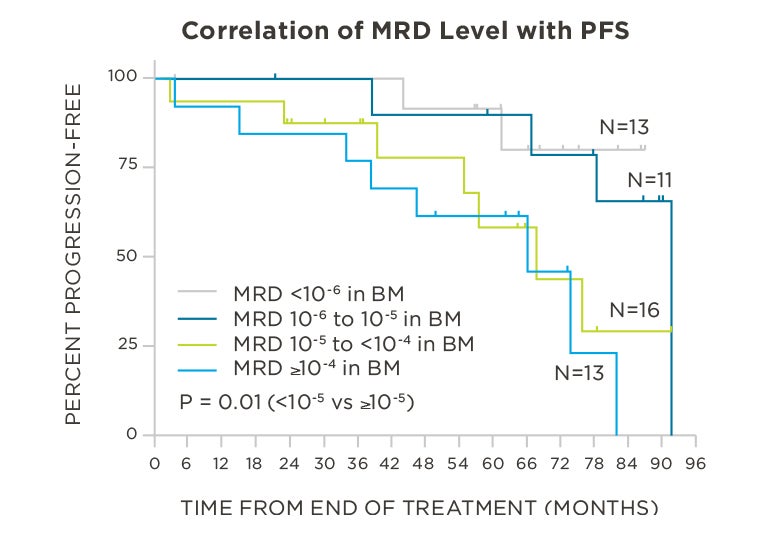
In bone marrow samples, clonoSEQ is predictive of PFS
Thompson et al assessed 62 previously untreated CLL patients who received therapy with fludarabine, cyclophosphomide, and rituximab (FCR). These patients were initially determined to be U-MRD by 4-color flow cytometry at an MRD threshold of 10-4. From these patients, 57 bone marrow (BM) samples were evaluated at the end of treatment by clonoSEQ. Patients who achieved the lowest levels of MRD in the bone marrow (10-5 – 10-6) or who had a U-MRD status (<10-6) experienced the best outcomes. Patients who had a U-MRD status at a threshold of < 10-5 had superior PFS compared to patients with MRD ≥ 10-5 (P = 0.01; Figure 3).[17]
clonoSEQ predicts outcomes in both blood and bone marrow
An expanded analysis of the Thompson et al data set supported the clinical validation of clonoSEQ. This data shows a significant association between PFS and continuous clonoSEQ MRD measurement (vs. at a pre-specified sensitivity threshold) in both blood and bone marrow, after end of treatment (P= 9.6x 10-4 for blood; P= 2.13 x 10-4 for bone marrow). Additionally, patients who had U-MRD status at a threshold < 10-6 had superior PFS compared to patients with MRD ≥ 10-6 (P = 7.74 x 10-2 for blood, Figure 4A; and P = 8.10 x 10-2 for bone marrow, Figure 4B).[1]
This page is intended for use by healthcare professionals outside of the United States.
The clonoSEQ Assay B-cell Reagent Set is an in vitro diagnostic that identifies and quantifies rearranged B-cell receptor gene sequences in DNA extracted from blood and bone marrow.
It is a manual test that determines measurable/minimal residual disease (MRD) and monitors changes in disease burden during and after treatment in B-cell malignancies. The test is indicated for use by qualified healthcare professionals for clinical decision-making and in conjunction with other clinicopathological features.
The clonoSEQ Assay is being utilized for a variety of investigator-sponsored clinical trials in B-cell lymphoid cancers. If you are interested in learning more about use of clonoSEQ in your own trials, contact dxsupport@adaptivebiotech.com.
Download CLL Clinical Data
Download our Chronic Lymphocytic Leukemia clinical data summary to explore and share the data.
VIEW PDFReview NCCN Guidelines®
Access the NCCN Guidelines.
GUIDELINESMedical Affairs inquiries
Make an inquiry to learn more about our products.
Citations
- clonoSEQ®. [technical summary]. Seattle, WA: Adaptive Biotechnologies; 2020. https://clonoseq.com/technical-summary.
- Perrot A, et al. Blood. 2018;132(23):2456-2464.
- Wood B, et al. Blood. 2018;131(12):1350-1359.
- Kumar S, et al. Lancet Oncol. 2016;17(8):e328-e346.
- Mateos M, et al. N Engl J Med. 2018;378(6):518-528.
- DARZALEX® Prescribing Information. Horsham, PA: Janssen Biotech, Inc; 2018.
- Dimopoulos M, et al. N Engl J Med. 2016;375(14):1319-31.
- Martinez-Lopez J, et al. Blood. 2014;123(20):3073-3079.
- Avet Loiseau H, et al. ASH 2015: Abstract 191.
- Referenced with permission from the NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®) for Multiple Myeloma V.3.2020. © National Comprehensive Cancer Network, Inc. 2020. All rights reserved. Accessed March 11th, 2020. To view the most recent and complete version of the guideline, go to NCCN.org.
- Moreau P, et al. Ann Oncol. 2017;00:1-11.
- Faham M, et al. Blood. 2012;120(26):5173-5180. (study author was an employee of Adaptive at time of publishing)
- Pulsipher M, et al. Blood. 2015;125(22):3501-8.
- Referenced with permission from the NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®) for Pediatric Acute Lymphoblastic Leukemia V.2.2020. © National Comprehensive Cancer Network, Inc. 2020. All rights reserved. Accessed March 11th, 2020. To view the most recent and complete version of the guideline, go to NCCN.org.
- Referenced with permission from the NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®) for Acute Lymphoblastic Leukemia V.1.2020. © National Comprehensive Cancer Network, Inc. 2020. All rights reserved. Accessed March 11th, 2020. To view the most recent and complete version of the guideline, go to NCCN.org.
- Hoelzer D, et al. Ann Oncol. 2016;27 (suppl_5): v69-v82.
- Thompson P, et al. Blood. 201928;134(22):1951-1959.
- Referenced with permission from the NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®) for Chronic Lymphocytic Leukemia/Small Lymphocytic Leukemia V.4.2020. © National Comprehensive Cancer Network, Inc. 2020. All rights reserved. Accessed [February 19, 2020]. To view the most recent and complete version of the guideline, go online to NCCN.org.